 What signals the advent of a heart attack? Is the pain you have is from heartburn? It is critical that you get immediate help if you are suffering from heart attack. Learn all about heart attack including what you should do if a loved one is suspected of having a heart attack. Continue Reading >>
What signals the advent of a heart attack? Is the pain you have is from heartburn? It is critical that you get immediate help if you are suffering from heart attack. Learn all about heart attack including what you should do if a loved one is suspected of having a heart attack. Continue Reading >>
Showing posts with label Heart. Show all posts
Showing posts with label Heart. Show all posts
Monday, August 04, 2008
How To Recognize When You Have a Heart Attack?
What signals the advent of a heart attack? Is the pain you have is from heartburn? It is critical that you get immediate help if you are suffering from heart attack. Learn all about heart attack including what you should do if a loved one is suspected of having a heart attack. Continue Reading >>
Friday, May 02, 2008
Hypertension Takes Huge Toll in Developing Countries
 (HealthDay News) -- Roughly 80 percent of high blood pressure-related deaths in the world occur in developing nations, a new study by New Zealand researchers shows.
(HealthDay News) -- Roughly 80 percent of high blood pressure-related deaths in the world occur in developing nations, a new study by New Zealand researchers shows.Once regarded as a problem only in high-income countries, high blood pressure is now a global problem that affects both rich and poor nations, the researchers said.
The researchers calculated that 7.6 million premature deaths (about 13.5 percent of the worldwide total) and 92 million disability-adjusted life years (DALYS) -- 6 percent of the worldwide total -- among people over age 30 were caused by high blood pressure in 2001.
About 54 percent of strokes and 47 percent of heart disease cases were attributed to high blood pressure. About half of those cases occurred in people with hypertension (greater than 140 mm Hg systolic), while the remainder occurred in people with lesser degrees of high blood pressure.
In high-income countries, the proportion of premature deaths due to high blood pressure was 17.6 percent, compared to 12.9 percent in middle- and low-income nations. The proportion of DALYS due to high blood pressure in high-income nations was 9.3 percent, compared to 5.6 percent in middle- and low-income nations.
However, 80 percent of worldwide high blood pressure-related deaths occurred in middle- and low-income nations in eastern Europe and Asia, including China and India. More than one-third of all deaths in lower-income nations in Europe and central Asia were related to high blood pressure.
In high-income countries there were 1.39 million high blood pressure-related deaths; 418,000 stroke deaths; 668,000 heart disease deaths; 109,000 deaths due to hypertensive disease; and 197,000 deaths due to other cardiovascular diseases.
In low- and middle-income countries, there were 6.22 million high blood pressure-related deaths: 2.5 million stroke deaths; 2.68 million heart disease deaths; 598,000 hypertensive disease deaths; and 445,000 deaths due to other cardiovascular diseases.
"Most of the disease burden caused by high blood pressure is borne by low-income and middle-income countries, by people in middle age, and by people with lesser degrees of high blood pressure. Prevention and treatment strategies restricted to rich countries or individuals with hypertension will miss much blood pressure-related disease," wrote the University of Auckland researchers.
The study is published in this week's issue of The Lancet.
"Middle-income countries and low-income regions have a five times greater burden of disease than high-income regions, with access to less than 10 percent of the global treatment resource... This travesty cannot continue to be ignored by those most able to bring about change," Stephen MacMahon, of the George Institute for International Health at the University of Sydney in Australia, and his international colleagues, wrote in an accompanying editorial.
More information
The American Heart Association has more about high blood pressure.
Friday, April 04, 2008
5 Ways to Boost Your Metabolism and Lose Weight
Magnesium, interval training, and other tricks to burn more calories
by Ross Weale
Health magazine contributor Samantha Heller shows how to burn more calories, during an interview on the Today show, March 10.
SAMANTHA HELLER
Samantha Heller, RD, is the nutrition coordinator at the Fairfield Connecticut YMCA. A certified dietitian/nutritionist and exercise physiologist, Heller earned her master's degree in nutrition and applied physiology from Teachers’ College, Columbia University. She served as the senior clinical nutritionist and exercise physiologist at NYU Medical center in New York City for almost a decade and created and ran the outpatient nutrition program for the NYU Cardiac Rehabilitation Program. She has also been a fitness instructor for 15 years. Heller specializes in nutrition, wellness, stress management, and fitness for people who are fighting heart disease, diabetes, cancer, and obesity.
A contributing editor to Health magazine, her writing has also appeared in numerous other magazines, including Men’s Fitness, Men’s Health, and Glamour, as well as sites such as Fitness.com.
by Ross Weale
Health magazine contributor Samantha Heller shows how to burn more calories, during an interview on the Today show, March 10.
SAMANTHA HELLER
Samantha Heller, RD, is the nutrition coordinator at the Fairfield Connecticut YMCA. A certified dietitian/nutritionist and exercise physiologist, Heller earned her master's degree in nutrition and applied physiology from Teachers’ College, Columbia University. She served as the senior clinical nutritionist and exercise physiologist at NYU Medical center in New York City for almost a decade and created and ran the outpatient nutrition program for the NYU Cardiac Rehabilitation Program. She has also been a fitness instructor for 15 years. Heller specializes in nutrition, wellness, stress management, and fitness for people who are fighting heart disease, diabetes, cancer, and obesity.
A contributing editor to Health magazine, her writing has also appeared in numerous other magazines, including Men’s Fitness, Men’s Health, and Glamour, as well as sites such as Fitness.com.
Tuesday, April 01, 2008
Will Your New House Make You Sick?
 The one we almost bought harbored cancer-causing gas and toxic mold. What buyers must check before their dream home turns into a nightmare
The one we almost bought harbored cancer-causing gas and toxic mold. What buyers must check before their dream home turns into a nightmareby Amy O'Connor
It was love at first sight. My husband and I couldn’t believe our luck. We met The One so early in our home-hunting process; the house was everything we’d ever dreamed of and more: neat and tidy, wrapped up in a bow.
Or so we thought when we offered asking price and had it accepted. We even bonded with the sweet little-old-lady seller, whose grandmotherly demeanor filled us with confidence about our impending purchase. I envisioned our closing date through a Vaseline-coated lens, complete with baked-from-scratch chocolate chip cookies provided by her and a group hug with both attorneys. Continue reading »
Thursday, March 27, 2008
Calcium Scans Help Predict Coronary Risk
 (HealthDay News) -- Scanning the heart arteries for calcium deposits can help predict future cardiac problems, a new study shows, but experts aren't sure that adding such scans to routine checkups would be worth the cost.
(HealthDay News) -- Scanning the heart arteries for calcium deposits can help predict future cardiac problems, a new study shows, but experts aren't sure that adding such scans to routine checkups would be worth the cost."It has been shown to be predictive" of potential heart trouble, said Dr. Diane Bild, deputy director of the division of prevention and population sciences at the U.S. National Heart, Lung, and Blood Institute, which funded the study. "Whether it is actually beneficial to the people who are screened has not been shown."
A calcium scan using computed tomography (CT) costs $300 to $600. These scans look for calcification -- hardening of the arteries caused by high blood fats and calcium deposits that can eventually cause blood vessel blockage. The scan is a potential competitor for much less expensive tests for coronary risk, such as blood cholesterol and blood pressure readings.
The new study involved more than 6,700 American men and women across a number of racial and ethnic groups -- white, black, Chinese, Hispanic -- who were followed for an average of 3.8 years. It found that the risk of a coronary event was nearly 10 times higher for those with the highest calcium deposit scores than for those with the lowest.
"This study was launched in 1999, a time when there was a lot of interest in whether this new test could predict coronary artery disease," Bild said. "A lot of studies have been done in predominantly white populations. This was one of our efforts to include minority groups."
The study does show that calcium scanning "modestly improves predictions over traditional risk factors," she said. "Several pieces of information are needed in order to understand whether this is clinically useful."
The findings are published in the March 27 issue of the New England Journal of Medicine.
The cost of such scans could be reduced, according to a statement from study lead author Dr. Robert Detrano, professor of radiological sciences at the University of California, Irvine, who is traveling in China. Scans have been done for just $30 in China, Detrano noted.
"It is mostly an issue of cost," said Dr. William S. Weintraub, chief of cardiology at the Christiana Health Care System, the largest health-care system in Delaware, who wrote an accompanying editorial in the journal. "It does add to our discrimination, but it costs a couple of hundred dollars and we're not sure how you use it."
Reducing the cost would make the test more usable, and "more epidemiological studies showing its value in risk prediction would be of great value," Weintraub said.
"But I'd be uncomfortable now with the idea of recommending this for everybody, or even defining a middle ground where we are unsure how we treat people so they get this first," he said.
A calcium scan also carries some risk, since it exposes a person to radiation, Bild noted. "It would be worth it if the benefit outweighed that risk," she said. "We don't clearly have both sides of that equation established."
More information
For more on coronary calcium scans, visit the U.S. Heart, Lung, and Blood Institute.
more discussion: Forum· Addiction Forum · Ask the Doctors Forum · Ayurveda Forum · Ayurvedic & Thai Herbs Forum · Colon Cleansing Forum · Dental Forum · Diabetes Forum · Diet Forum · General Cleansing Forum · Hepatitis A, B. C Forum · Integrated Medicine Forum · Live Blood Analysis Forum · Ozone-Oxygen-Forum · pH - Alkaline - Acidity Forum · Weight Loss Forum
Friday, March 21, 2008
A good marriage could be the key to better blood pressure
Story Highlights:

That second finding is a surprise because prior studies have shown that married people tend to be healthier than singles, said researcher Julianne Holt-Lunstad.
It would take further study to sort out what the results mean for long-term health, said Holt-Lunstad, an assistant psychology professor at Brigham Young University.
Her study was reported online Thursday by the Annals of Behavioral Medicine.
The study involved 204 married people and 99 single adults. Most were white, and it's not clear whether the same results would apply to other ethnic groups, Holt-Lunstad said.
Study volunteers wore devices that recorded their blood pressure at random times over 24 hours. Married participants also filled out questionnaires about their marriage.
Analysis found that the more marital satisfaction and adjustment spouses reported, the lower their average blood pressure was over the 24 hours and during the daytime.
But spouses who scored low in marital satisfaction had higher average blood pressure than single people did.
During the daytime, their average was about five points higher, entering a range that's considered a warning sign. (That result is for the top number in a blood pressure reading).
"I think this (study) is worth some attention," said Karen Matthews, a professor of psychiatry, psychology and epidemiology at the University of Pittsburgh. She studies heart disease and high blood pressure but didn't participate in the new work.
Few studies of the risk for high blood pressure have looked at marital quality rather than just marital status, she said.
It makes sense that marital quality is more important than just being married when it comes to affecting blood pressure, said Dr. Brian Baker, an associate professor of psychiatry at the University of Toronto.
- Most happily married people had better blood pressure, study showed
- Doctor: Marital quality more important than just being married
- Spouses with low marital satisfaction had higher blood pressure than singles
- Study involved mostly white people; not known if race is a factor
That second finding is a surprise because prior studies have shown that married people tend to be healthier than singles, said researcher Julianne Holt-Lunstad.
It would take further study to sort out what the results mean for long-term health, said Holt-Lunstad, an assistant psychology professor at Brigham Young University.
Her study was reported online Thursday by the Annals of Behavioral Medicine.
The study involved 204 married people and 99 single adults. Most were white, and it's not clear whether the same results would apply to other ethnic groups, Holt-Lunstad said.
Study volunteers wore devices that recorded their blood pressure at random times over 24 hours. Married participants also filled out questionnaires about their marriage.
Analysis found that the more marital satisfaction and adjustment spouses reported, the lower their average blood pressure was over the 24 hours and during the daytime.
But spouses who scored low in marital satisfaction had higher average blood pressure than single people did.
During the daytime, their average was about five points higher, entering a range that's considered a warning sign. (That result is for the top number in a blood pressure reading).
"I think this (study) is worth some attention," said Karen Matthews, a professor of psychiatry, psychology and epidemiology at the University of Pittsburgh. She studies heart disease and high blood pressure but didn't participate in the new work.
Few studies of the risk for high blood pressure have looked at marital quality rather than just marital status, she said.
It makes sense that marital quality is more important than just being married when it comes to affecting blood pressure, said Dr. Brian Baker, an associate professor of psychiatry at the University of Toronto.
Tuesday, December 11, 2007
Hypertension Linked to Risk of Mild Cognitive Impairment
(HealthDay News) -- High blood pressure may be associated with increased risk for mild cognitive impairment, says a study by researchers at the Columbia University Medical Center in New York City.
Mild cognitive impairment, which causes learning and thinking difficulties, has "attracted increasing interest during the past years, particularly as a means of identifying the early stages of Alzheimer's disease as a target for treatment and prevention," the study authors wrote.
They followed 918 Medicare recipients aged 65 and older (average age 76.3) who were assessed every 18 months for an average of 4.7 years. None of the participants had mild cognitive impairment at the start of the study, but 334 of them developed the condition during the study period.
Of those, 160 developed amnestic mild cognitive impairment (which involves low scores on memory portions of neuropsychological tests), and 174 developed non-amnestic mild cognitive impairment. Hypertension was associated with an increased risk of all types of mild cognitive impairment, especially non-amnestic mild cognitive impairment, the researchers said.
The findings are published in the December issue of the Archives of Neurology.
"The mechanism by which blood pressure affects the risk of cognitive impairment or dementia remains unclear. Hypertension may cause cognitive impairment through cerebrovascular disease. Hypertension is a risk factor for subcortical white matter lesions found commonly in Alzheimer's disease. Hypertension may also contribute to a blood-brain barrier dysfunction, which has been suggested to be involved in the cause of Alzheimer's disease.
Other possible explanations for the association are shared risk factors," including the formation of cell-damaging compounds known as free radicals, the study authors wrote.
"Our findings support the hypothesis that hypertension increases the risk of incident mild cognitive impairment, especially non-amnestic mild cognitive impairment," the researchers concluded. "Preventing and treating hypertension may have an important impact in lowering the risk of cognitive impairment."
More information
The Alzheimer's Association has more about mild cognitive impairment.
Mild cognitive impairment, which causes learning and thinking difficulties, has "attracted increasing interest during the past years, particularly as a means of identifying the early stages of Alzheimer's disease as a target for treatment and prevention," the study authors wrote.
They followed 918 Medicare recipients aged 65 and older (average age 76.3) who were assessed every 18 months for an average of 4.7 years. None of the participants had mild cognitive impairment at the start of the study, but 334 of them developed the condition during the study period.
Of those, 160 developed amnestic mild cognitive impairment (which involves low scores on memory portions of neuropsychological tests), and 174 developed non-amnestic mild cognitive impairment. Hypertension was associated with an increased risk of all types of mild cognitive impairment, especially non-amnestic mild cognitive impairment, the researchers said.
The findings are published in the December issue of the Archives of Neurology.
"The mechanism by which blood pressure affects the risk of cognitive impairment or dementia remains unclear. Hypertension may cause cognitive impairment through cerebrovascular disease. Hypertension is a risk factor for subcortical white matter lesions found commonly in Alzheimer's disease. Hypertension may also contribute to a blood-brain barrier dysfunction, which has been suggested to be involved in the cause of Alzheimer's disease.
Other possible explanations for the association are shared risk factors," including the formation of cell-damaging compounds known as free radicals, the study authors wrote.
"Our findings support the hypothesis that hypertension increases the risk of incident mild cognitive impairment, especially non-amnestic mild cognitive impairment," the researchers concluded. "Preventing and treating hypertension may have an important impact in lowering the risk of cognitive impairment."
More information
The Alzheimer's Association has more about mild cognitive impairment.
Tuesday, October 09, 2007
Cardiac Artery Trouble Boosts Family Heart Risk
(HealthDay News) -- The close relatives of people who carry an abnormality in the heart's left main artery should take special care of their own cardiac health, experts say.
Healthy brothers and sisters of someone with such problems are 2.5 times more likely to develop some form of heart disease, compared to the siblings of patients with heart disease not related to that artery, concludes a report in the Oct. 4 issue of the European Heart Journal.
"We first reported a relationship two years ago," said Dr. Heribert Schunkert, head of cardiology at the University of Luebeck, Germany, and lead author of two reports in the journal. "This time, we specifically investigated the possibility of high heritability of the condition. That was the case."
In one report, Schunkert and his colleagues analyzed coronary angiograms from more than 1,800 members of families in which two or more people developed coronary artery disease.
They found that 12 percent had a 50 percent or more narrowing of the left main coronary artery. According to Schunkert, that finding demonstrated that the problem clusters in families and that its cause was probably genetic.
The second study followed almost 1,400 healthy brothers and sisters of people with coronary artery disease for five years.
A left main coronary artery problem was found in 13.9 percent of those who developed heart disease but in only 6.4 percent of those who did not. The risk of developing heart disease was 2.5 times higher for brothers and sisters of someone with a left coronary artery than in those where the patient suffered from some other form of heart disease.
"The clinical implication is that if a person demonstrates a left main coronary artery problem, siblings should know that they have a greatly increased risk of coronary artery disease," Schunkert said.
Those family members might undergo screening to detect left main coronary artery problems, he said, although it is not clear whether the chance of preventing heart disease is high enough to justify the costs and risks of screening.
But the German studies do not necessarily show that problems with the left main coronary artery gives relatives any more reason be concerned, said Dr. Dhananjay Vaidya, an assistant professor of internal medicine at the Johns Hopkins University in Baltimore.
Because a family history of heart disease is a known risk factor for heart trouble, "brothers and sisters of someone with any heart disease should take it seriously," said Vaidya, who is also a member of the team conducting the Sibling Family Heart Study.
The Sibling Family Heart Study has enrolled more than 700 family members of people treated for heart attacks in Baltimore hospitals. Researchers are following them to detect "whether persons present with the same kind of heart disease as their close relatives," Vaidya said.
There is particular reason to worry when the left main coronary artery is affected, since it supplies about two-thirds of the heart's blood flow, Vaidya said. But the German studies showed that this was a relatively rare condition, and the data on its heritability was not conclusive, he said.
It's possible that the Baltimore study may now be changed slightly "to determine if there is something biologically special about left main coronary artery disease," Vaidya said.
More information
The role of family history in the various risk factors for heart disease is explained by the American Heart Association.
Healthy brothers and sisters of someone with such problems are 2.5 times more likely to develop some form of heart disease, compared to the siblings of patients with heart disease not related to that artery, concludes a report in the Oct. 4 issue of the European Heart Journal.
"We first reported a relationship two years ago," said Dr. Heribert Schunkert, head of cardiology at the University of Luebeck, Germany, and lead author of two reports in the journal. "This time, we specifically investigated the possibility of high heritability of the condition. That was the case."
In one report, Schunkert and his colleagues analyzed coronary angiograms from more than 1,800 members of families in which two or more people developed coronary artery disease.
They found that 12 percent had a 50 percent or more narrowing of the left main coronary artery. According to Schunkert, that finding demonstrated that the problem clusters in families and that its cause was probably genetic.
The second study followed almost 1,400 healthy brothers and sisters of people with coronary artery disease for five years.
A left main coronary artery problem was found in 13.9 percent of those who developed heart disease but in only 6.4 percent of those who did not. The risk of developing heart disease was 2.5 times higher for brothers and sisters of someone with a left coronary artery than in those where the patient suffered from some other form of heart disease.
"The clinical implication is that if a person demonstrates a left main coronary artery problem, siblings should know that they have a greatly increased risk of coronary artery disease," Schunkert said.
Those family members might undergo screening to detect left main coronary artery problems, he said, although it is not clear whether the chance of preventing heart disease is high enough to justify the costs and risks of screening.
But the German studies do not necessarily show that problems with the left main coronary artery gives relatives any more reason be concerned, said Dr. Dhananjay Vaidya, an assistant professor of internal medicine at the Johns Hopkins University in Baltimore.
Because a family history of heart disease is a known risk factor for heart trouble, "brothers and sisters of someone with any heart disease should take it seriously," said Vaidya, who is also a member of the team conducting the Sibling Family Heart Study.
The Sibling Family Heart Study has enrolled more than 700 family members of people treated for heart attacks in Baltimore hospitals. Researchers are following them to detect "whether persons present with the same kind of heart disease as their close relatives," Vaidya said.
There is particular reason to worry when the left main coronary artery is affected, since it supplies about two-thirds of the heart's blood flow, Vaidya said. But the German studies showed that this was a relatively rare condition, and the data on its heritability was not conclusive, he said.
It's possible that the Baltimore study may now be changed slightly "to determine if there is something biologically special about left main coronary artery disease," Vaidya said.
More information
The role of family history in the various risk factors for heart disease is explained by the American Heart Association.
Sunday, September 30, 2007
Weight Loss Can Control Hypertension
(HealthDay News) -- An Italian study has identified overweight as a direct cause of high blood pressure. And it also showed that up to half of overweight people can bring down blood pressure to healthy levels by weight reduction.
But the weight loss has to be achieved before the borderline to outright obesity is crossed, said Dr. Roberto Fogari, professor of medicine at the University of Pavia. He was to present the study findings Friday at the annual meeting of the American Heart Association's Council for High Blood Pressure Research, in Tucson, Ariz.
It's important that the study linked overweight to high blood pressure, which usually is described as "essential," a medical term meaning that the cause is unknown, Fogari said.
"The study suggests that, in many cases, hypertension [high blood pressure] is not essential," he said. "It is secondary to overweight. So, in the first stages of overweight, if we can induce people to reduce overweight, they can also avoid being treated for hypertension."
The study included 210 men and women whose body mass index [a ratio of weight to height] was between 25 and 29.9, indicating overweight but just short of the 30 mark of obesity. Their systolic blood pressure was between 140 and 159, and their diastolic pressure was between 90 and 99, indicating moderately high blood pressure.
An individualized low-calorie diet was designed for each study participant. Some also were prescribed orlistat, a drug that prevents fat from being metabolized.
After six months, 53 percent of the men and 49 percent of the women in the study achieved normal body weight, and a 5 percent reduction in blood pressure.
"The other 50 percent of those in the study already had abnormal changes in the vascular tree [blood vessel system], so that hypertension was no longer reversible by losing weight," Fogari said.
The implication for practicing physicians who see moderately overweight people with high blood pressure is that their first goal should be weight reduction, he said.
"Only after six months of trying to reduce the patient's weight can a decision be made about drug treatment," Fogari said.
Dr. Daniel W. Jones, dean of the University of Mississippi School of Medicine, and a spokesman for the American Heart Association, said the study finding "is not new news, but it is important news."
There have been a number of previous studies showing that weight loss can reduce blood pressure, Jones said. "But this is an increasingly important problem in societies around the world," he said. "Once you gain weight, you find it difficult to lose weight, which is why we focus so much on preventing obesity these days."
As for drug treatment of high blood pressure, about half of California adults diagnosed with hypertension do not take medication for it, another report presented at the same meeting found.
The study of 11,467 persons given a diagnosis of hypertension found that 49.4 percent were not taking drugs to reduce their blood pressure, said the report by researchers at the California Department of Public Health's Heart Disease and Stroke Prevention Program.
There were some bright spots in the picture. Compliance was more than five times higher for those who had seen a doctor in the past year than for those who had not. And the compliance rate was twice as high for persons with health insurance than the uninsured.
More information
For more on high blood pressure and what to do about it, turn to the American Heart Association.
But the weight loss has to be achieved before the borderline to outright obesity is crossed, said Dr. Roberto Fogari, professor of medicine at the University of Pavia. He was to present the study findings Friday at the annual meeting of the American Heart Association's Council for High Blood Pressure Research, in Tucson, Ariz.
It's important that the study linked overweight to high blood pressure, which usually is described as "essential," a medical term meaning that the cause is unknown, Fogari said.
"The study suggests that, in many cases, hypertension [high blood pressure] is not essential," he said. "It is secondary to overweight. So, in the first stages of overweight, if we can induce people to reduce overweight, they can also avoid being treated for hypertension."
The study included 210 men and women whose body mass index [a ratio of weight to height] was between 25 and 29.9, indicating overweight but just short of the 30 mark of obesity. Their systolic blood pressure was between 140 and 159, and their diastolic pressure was between 90 and 99, indicating moderately high blood pressure.
An individualized low-calorie diet was designed for each study participant. Some also were prescribed orlistat, a drug that prevents fat from being metabolized.
After six months, 53 percent of the men and 49 percent of the women in the study achieved normal body weight, and a 5 percent reduction in blood pressure.
"The other 50 percent of those in the study already had abnormal changes in the vascular tree [blood vessel system], so that hypertension was no longer reversible by losing weight," Fogari said.
The implication for practicing physicians who see moderately overweight people with high blood pressure is that their first goal should be weight reduction, he said.
"Only after six months of trying to reduce the patient's weight can a decision be made about drug treatment," Fogari said.
Dr. Daniel W. Jones, dean of the University of Mississippi School of Medicine, and a spokesman for the American Heart Association, said the study finding "is not new news, but it is important news."
There have been a number of previous studies showing that weight loss can reduce blood pressure, Jones said. "But this is an increasingly important problem in societies around the world," he said. "Once you gain weight, you find it difficult to lose weight, which is why we focus so much on preventing obesity these days."
As for drug treatment of high blood pressure, about half of California adults diagnosed with hypertension do not take medication for it, another report presented at the same meeting found.
The study of 11,467 persons given a diagnosis of hypertension found that 49.4 percent were not taking drugs to reduce their blood pressure, said the report by researchers at the California Department of Public Health's Heart Disease and Stroke Prevention Program.
There were some bright spots in the picture. Compliance was more than five times higher for those who had seen a doctor in the past year than for those who had not. And the compliance rate was twice as high for persons with health insurance than the uninsured.
More information
For more on high blood pressure and what to do about it, turn to the American Heart Association.
Sunday, July 29, 2007
Blood Pressure Drop During Bypass Might Impair Thinking
(HealthDay News) -- Patients who experience a blood pressure drop during bypass surgery may be at increased risk for a short-term dip in their cognitive abilities.
Researchers at the Johns Hopkins University School of Medicine in Baltimore studied 15 patients, aged 57 to 81, who were given cognitive tests before and then three to five days after they had coronary artery bypass graft (CABG) surgery.
All the patients had a decrease in mean arterial pressure (MAP) during surgery compared with their MAP before surgery. MAP provides doctors with an estimate of the blood pressure in various organs in the body.
The study found that patients whose MAP decreased by 27 millimeters of mercury or more had an average decrease of 1.4 points (out of a maximum of 30 points) on a standard cognitive test. Patients with a MAP decrease of less than 27 millimeters of mercury increased their scores by an average of one point.
Patients with a high MAP before their surgery were more likely to score lower on the cognitive test after their surgery.
The researchers also used MRI to examine the brains of 13 of the patients. They found that patients whose MAP decreased by more than 27 millimeters of mercury were 2.7 times more likely to show evidence of acute stroke.
The study was published online this week in the Archives of Neurology and is expected to be published in the August print issue.
The preliminary data from this small study suggests "that a substantial decrease in MAP from a patient's baseline may be a risk factor for short-term cognitive dysfunction," the study authors wrote. "This may be in part because of an increased risk for radiographic stroke."
Further studies are needed, the researchers said.
More information
The Alzheimer's Association has more about mild cognitive impairment.
Researchers at the Johns Hopkins University School of Medicine in Baltimore studied 15 patients, aged 57 to 81, who were given cognitive tests before and then three to five days after they had coronary artery bypass graft (CABG) surgery.
All the patients had a decrease in mean arterial pressure (MAP) during surgery compared with their MAP before surgery. MAP provides doctors with an estimate of the blood pressure in various organs in the body.
The study found that patients whose MAP decreased by 27 millimeters of mercury or more had an average decrease of 1.4 points (out of a maximum of 30 points) on a standard cognitive test. Patients with a MAP decrease of less than 27 millimeters of mercury increased their scores by an average of one point.
Patients with a high MAP before their surgery were more likely to score lower on the cognitive test after their surgery.
The researchers also used MRI to examine the brains of 13 of the patients. They found that patients whose MAP decreased by more than 27 millimeters of mercury were 2.7 times more likely to show evidence of acute stroke.
The study was published online this week in the Archives of Neurology and is expected to be published in the August print issue.
The preliminary data from this small study suggests "that a substantial decrease in MAP from a patient's baseline may be a risk factor for short-term cognitive dysfunction," the study authors wrote. "This may be in part because of an increased risk for radiographic stroke."
Further studies are needed, the researchers said.
More information
The Alzheimer's Association has more about mild cognitive impairment.
Thursday, July 05, 2007
Don't Get Burned by Heat Stroke
(HealthDay News) -- Staying cool on hot summer days isn't just comfortable, it could save your life, according to the Pennsylvania Medical Society.
Heat stroke -- injury to internal organs caused by an excessively high body temperature -- is a serious and potentially deadly illness that can usually be prevented. Even so, it still happens all too frequently, experts say.
Many people recall the August 2001 death of Minnesota Viking's football player Korey Stringer.
He died after developing multi-organ system failure on a hot day. Athletes are particularly vulnerable to heat stroke -- especially football players, who wear body-covering uniforms and practice in the hottest temperatures -- but it can affect anyone.
Heat stroke can occur when you are in an extremely hot environment for a long period of time. It also happens when people overexert themselves on very hot days.
According to the Pennsylvania Medical Society, you should be alert to heat stroke on days when the relative humidity is at least 70 percent and temperatures are 95 degrees Fahrenheit and higher.
Other heat-related afflictions that may be a sign of looming heat stroke include heat cramps and heat exhaustion, which is characterized by pale, moist skin; headache; dizziness; nausea;
increased heart rate; low blood pressure; elevated temperature and profuse sweating.
The symptoms of heat stroke are more severe than those of heat exhaustion and may include:
Initial profuse sweating.
Hot, dry red skin.
High fever.
Vomiting.
Confusion.
Seizures during cooling.
Unconsciousness.
Sometimes lack of sweating, though athletes may perspire.
High body temperature (often 105 degrees or higher).
Anyone experiencing these symptoms should immediately seek emergency medical help.
Steps you can take to keep cool despite hot temperatures include:
Avoid overexertion.
Drink a quart of fluids an hour.
Wear loose, light-colored clothing made of light fabrics.
Wear a hat and sunblock.
Stay in the shade or indoors when possible.
Open windows and use fans and/or air conditioning; if you don't have air conditioning, go to a public place that does (a mall, library or movie theater).
Avoid dehydrating beverages such as caffeine and alcohol.
More information
The U.S. Centers for Disease Control and Prevention has more about extreme heat.
Heat stroke -- injury to internal organs caused by an excessively high body temperature -- is a serious and potentially deadly illness that can usually be prevented. Even so, it still happens all too frequently, experts say.
Many people recall the August 2001 death of Minnesota Viking's football player Korey Stringer.
He died after developing multi-organ system failure on a hot day. Athletes are particularly vulnerable to heat stroke -- especially football players, who wear body-covering uniforms and practice in the hottest temperatures -- but it can affect anyone.
Heat stroke can occur when you are in an extremely hot environment for a long period of time. It also happens when people overexert themselves on very hot days.
According to the Pennsylvania Medical Society, you should be alert to heat stroke on days when the relative humidity is at least 70 percent and temperatures are 95 degrees Fahrenheit and higher.
Other heat-related afflictions that may be a sign of looming heat stroke include heat cramps and heat exhaustion, which is characterized by pale, moist skin; headache; dizziness; nausea;
increased heart rate; low blood pressure; elevated temperature and profuse sweating.
The symptoms of heat stroke are more severe than those of heat exhaustion and may include:
Initial profuse sweating.
Hot, dry red skin.
High fever.
Vomiting.
Confusion.
Seizures during cooling.
Unconsciousness.
Sometimes lack of sweating, though athletes may perspire.
High body temperature (often 105 degrees or higher).
Anyone experiencing these symptoms should immediately seek emergency medical help.
Steps you can take to keep cool despite hot temperatures include:
Avoid overexertion.
Drink a quart of fluids an hour.
Wear loose, light-colored clothing made of light fabrics.
Wear a hat and sunblock.
Stay in the shade or indoors when possible.
Open windows and use fans and/or air conditioning; if you don't have air conditioning, go to a public place that does (a mall, library or movie theater).
Avoid dehydrating beverages such as caffeine and alcohol.
More information
The U.S. Centers for Disease Control and Prevention has more about extreme heat.
Saturday, June 02, 2007
Biodegradable Stent Successful in Human Trial
(HealthDay News) -- A stent that biodegrades and vanishes from an artery in a matter of months has successfully passed a major test in humans, German researchers report.
The device, made of magnesium, is one of many different biodegradable stents that together represent the future of these artery-opening devices, said Dr. Raimund Erbel, professor of medicine at the West German Heart Center in Essen, and lead author of a report on the trial in the June 2 issue of The Lancet.
Stents are tiny, implanted mesh tubes that prop open failing arteries.
"In the long run, a biodegradable stent is best for those who need a coronary stent," Erbel said. "When such a stent has done its job, you don't need it any more. In the long run, its presence can cause problems."
A number of cardiologists and companies in countries across the world are working to develop stents that are broken down by the body once they have succeeded in keeping blood flowing through an artery. Most of this work is going on outside the United States, with reports on early trials coming from China, Japan, Finland, Germany, and elsewhere.
For example, at a heart meeting earlier this year, a group at Erasmus University in Amsterdam reported on a biodegradable stent they placed in 30 cardiac patients. The devices behaved very much like standard metal stents over the relatively brief period of a month, the researchers reported. The patients are still being followed to determine exactly when and how the stents disappear.
In this new trial, Erbel and his colleagues implanted 71 magnesium stents in 63 patients.
They reported that the safety record of the devices remained good after 12 months, with not a single case of clotting noted within the stent and no incidents of heart attack or death among patients. The diameter of the treated arteries increased slightly as the magnesium was absorbed by the body, being replaced by natural calcium and phosphorus.
As a bonus, the patients did not require treatment with clot-dissolving drugs such as Plavix and aspirin -- medicines that are typically needed with today's permanent metal stents.
The magnesium devices were far from perfect, however. Re-blockage of an artery occurred in 47.5 percent of patients, with 27 percent of them requiring artery-opening procedures.
One unexpected benefit of the magnesium stents was that it allowed the cardiologists to see what was happening inside the devices by using either MRI or CT scans. "Such views are hard to get with current devices, but we could get a wonderful visualization of an artery," Erbel said.
He views magnesium as a natural material for a degradable stent, because it is easily handled by the body. "After four months, everything is gone," Erbel said. "In fact, the degradation process was, in our opinion, too rapid, something we are researching," he said.
Joachim Kohn, director of the New Jersey Center for Biomaterials at Rutgers University, disagreed that biodegradable magnesium stents are the wave of the future.
"I'm familiar with this and don't think it will work very well, in spite of the early positive results," Kohn said. "We are going to see a number of complications in the end stages of the degradation of magnesium. It is a revolutionary and very innovative idea, but, in the end, we are better off with a body-like material than with a metal."
Kohn has developed a stent that uses just such a synthetic "biomaterial." It has been licensed to a small company, REVA Medical, with first human tests scheduled to begin this month.
Almost all the degradable stents now under development use such synthetic materials, which helps explain why so little is being done in the United States, Kohn said.
"Biomaterials were hot in the 1990s," he said. "Everyone in the United States was interested in biomaterials. But a field has to be matured, and before that happened, we moved on to other things, such as nanomaterials."
Wherever the work is done, "there is no question that we will want a biodegradable stent eventually," Kohn said. "There are persistent issues with permanent stents." It will take years to get such stents into routine medical use, he said, because careful human testing will be required.
More information
For more on stents, visit the American Heart Association.
The device, made of magnesium, is one of many different biodegradable stents that together represent the future of these artery-opening devices, said Dr. Raimund Erbel, professor of medicine at the West German Heart Center in Essen, and lead author of a report on the trial in the June 2 issue of The Lancet.
Stents are tiny, implanted mesh tubes that prop open failing arteries.
"In the long run, a biodegradable stent is best for those who need a coronary stent," Erbel said. "When such a stent has done its job, you don't need it any more. In the long run, its presence can cause problems."
A number of cardiologists and companies in countries across the world are working to develop stents that are broken down by the body once they have succeeded in keeping blood flowing through an artery. Most of this work is going on outside the United States, with reports on early trials coming from China, Japan, Finland, Germany, and elsewhere.
For example, at a heart meeting earlier this year, a group at Erasmus University in Amsterdam reported on a biodegradable stent they placed in 30 cardiac patients. The devices behaved very much like standard metal stents over the relatively brief period of a month, the researchers reported. The patients are still being followed to determine exactly when and how the stents disappear.
In this new trial, Erbel and his colleagues implanted 71 magnesium stents in 63 patients.
They reported that the safety record of the devices remained good after 12 months, with not a single case of clotting noted within the stent and no incidents of heart attack or death among patients. The diameter of the treated arteries increased slightly as the magnesium was absorbed by the body, being replaced by natural calcium and phosphorus.
As a bonus, the patients did not require treatment with clot-dissolving drugs such as Plavix and aspirin -- medicines that are typically needed with today's permanent metal stents.
The magnesium devices were far from perfect, however. Re-blockage of an artery occurred in 47.5 percent of patients, with 27 percent of them requiring artery-opening procedures.
One unexpected benefit of the magnesium stents was that it allowed the cardiologists to see what was happening inside the devices by using either MRI or CT scans. "Such views are hard to get with current devices, but we could get a wonderful visualization of an artery," Erbel said.
He views magnesium as a natural material for a degradable stent, because it is easily handled by the body. "After four months, everything is gone," Erbel said. "In fact, the degradation process was, in our opinion, too rapid, something we are researching," he said.
Joachim Kohn, director of the New Jersey Center for Biomaterials at Rutgers University, disagreed that biodegradable magnesium stents are the wave of the future.
"I'm familiar with this and don't think it will work very well, in spite of the early positive results," Kohn said. "We are going to see a number of complications in the end stages of the degradation of magnesium. It is a revolutionary and very innovative idea, but, in the end, we are better off with a body-like material than with a metal."
Kohn has developed a stent that uses just such a synthetic "biomaterial." It has been licensed to a small company, REVA Medical, with first human tests scheduled to begin this month.
Almost all the degradable stents now under development use such synthetic materials, which helps explain why so little is being done in the United States, Kohn said.
"Biomaterials were hot in the 1990s," he said. "Everyone in the United States was interested in biomaterials. But a field has to be matured, and before that happened, we moved on to other things, such as nanomaterials."
Wherever the work is done, "there is no question that we will want a biodegradable stent eventually," Kohn said. "There are persistent issues with permanent stents." It will take years to get such stents into routine medical use, he said, because careful human testing will be required.
More information
For more on stents, visit the American Heart Association.
Monday, May 14, 2007
Pregnant women restricted to bed rest can and should do safe, specially-designed physical activity, say experts at the American Ph
(HealthDay News) -- Cardiologists should be giving more of the clot-preventing drug Plavix than is now recommended before performing the artery-opening procedure called angioplasty, a new study says.
The analysis of 10 previous studies found that giving angioplasty patients double the current recommended dose of Plavix -- 600 milligrams rather than 300 -- cut the combined risk of heart attack and cardiac death by half, according to Dr. Anthony Abbate.
Abbate, an assistant professor of medicine at Virginia Commonwealth University, was expected to present the findings on Friday at the Society for Cardiovascular Angiography and Interventions' annual meeting, in Orlando, Fla.
The higher dose did not increase the risk of serious bleeding, a major concern with Plavix, the analysis found.
"The evidence shown by this meta-analysis is very powerful," said Dr. Gregory Dehmer, president of the society and a professor of medicine at Texas A&M College of Medicine. "Although Plavix is powerful stuff, the meta-analysis did not find an excessive amount of bleeding. So we have a lower risk of myocardial infarction [heart attack] with no significant increase in adverse side effects."
The 10 studies analyzed by Abbate and Dr. Giuseppe G. Biondi-Zoccai, an assistant professor of cardiology at the University of Turin in Italy, included 1,500 patients who had angioplasty. Most had either 300 milligrams or 600 milligrams of Plavix before the procedure.
The incidence of cardiac death or nonfatal heart attack was 50 percent lower in the following 30 days in those getting the higher dose of Plavix. Only 3.1 percent of those getting the 600-milligram dose had in-hospital heart attacks, compared to 6.4 percent of those getting the 300-milligram dose. The overall 30-day incidence of death or heart attack was 3.8 percent for the higher dose and 7.3 percent for the lower dose, according to the study.
"This research has important clinical and cost implications," Biondi-Zoccai said in a prepared statement.
Current guidelines by the American Heart Association, the American College of Cardiology and the Society for Cardiovascular Angiography and Interventions say that physicians should "strongly consider" giving 300 milligrams of Plavix before angioplasty, a medical procedure to open narrowed or blocked blood vessels of the heart.
"Those guidelines are in the process of having an update," Dehmer said, adding that new guidelines are expected "in the next few months."
"In practical terms, many practitioners are concerned about the current recommendations," Dehmer said. "One concern is that should the patient require elective bypass surgery, does a higher dose of clopidogrel [the generic name of Plavix] increase the risk of excessive bleeding?
"Also there is the bleeding risk. It is addressed in this meta-analysis, which shows very minimal potential downside," he added.
But the final word is not in yet, said Dr. Marc S. Sabatine, associate professor in the cardiovascular division of Brigham and Women's Hospital in Boston. That will come from a major international study, to include up to 14,000 angioplasty patients, which is still enrolling participants, he said.
The smaller studies included in the current meta-analysis aren't definitive, Sabatine said, because there can be "publication bias," meaning that studies showing a positive result are more likely to get into print.
Timing also plays a role in treatment, he noted. Plavix must be activated in the liver, which takes about six hours, so giving it earlier makes it more effective.
But even with those side considerations, "many laboratories are considering switching to 600 milligrams," Sabatine said.
More information
For more on angioplasty, visit the U.S. National Library of Medicine.
The analysis of 10 previous studies found that giving angioplasty patients double the current recommended dose of Plavix -- 600 milligrams rather than 300 -- cut the combined risk of heart attack and cardiac death by half, according to Dr. Anthony Abbate.
Abbate, an assistant professor of medicine at Virginia Commonwealth University, was expected to present the findings on Friday at the Society for Cardiovascular Angiography and Interventions' annual meeting, in Orlando, Fla.
The higher dose did not increase the risk of serious bleeding, a major concern with Plavix, the analysis found.
"The evidence shown by this meta-analysis is very powerful," said Dr. Gregory Dehmer, president of the society and a professor of medicine at Texas A&M College of Medicine. "Although Plavix is powerful stuff, the meta-analysis did not find an excessive amount of bleeding. So we have a lower risk of myocardial infarction [heart attack] with no significant increase in adverse side effects."
The 10 studies analyzed by Abbate and Dr. Giuseppe G. Biondi-Zoccai, an assistant professor of cardiology at the University of Turin in Italy, included 1,500 patients who had angioplasty. Most had either 300 milligrams or 600 milligrams of Plavix before the procedure.
The incidence of cardiac death or nonfatal heart attack was 50 percent lower in the following 30 days in those getting the higher dose of Plavix. Only 3.1 percent of those getting the 600-milligram dose had in-hospital heart attacks, compared to 6.4 percent of those getting the 300-milligram dose. The overall 30-day incidence of death or heart attack was 3.8 percent for the higher dose and 7.3 percent for the lower dose, according to the study.
"This research has important clinical and cost implications," Biondi-Zoccai said in a prepared statement.
Current guidelines by the American Heart Association, the American College of Cardiology and the Society for Cardiovascular Angiography and Interventions say that physicians should "strongly consider" giving 300 milligrams of Plavix before angioplasty, a medical procedure to open narrowed or blocked blood vessels of the heart.
"Those guidelines are in the process of having an update," Dehmer said, adding that new guidelines are expected "in the next few months."
"In practical terms, many practitioners are concerned about the current recommendations," Dehmer said. "One concern is that should the patient require elective bypass surgery, does a higher dose of clopidogrel [the generic name of Plavix] increase the risk of excessive bleeding?
"Also there is the bleeding risk. It is addressed in this meta-analysis, which shows very minimal potential downside," he added.
But the final word is not in yet, said Dr. Marc S. Sabatine, associate professor in the cardiovascular division of Brigham and Women's Hospital in Boston. That will come from a major international study, to include up to 14,000 angioplasty patients, which is still enrolling participants, he said.
The smaller studies included in the current meta-analysis aren't definitive, Sabatine said, because there can be "publication bias," meaning that studies showing a positive result are more likely to get into print.
Timing also plays a role in treatment, he noted. Plavix must be activated in the liver, which takes about six hours, so giving it earlier makes it more effective.
But even with those side considerations, "many laboratories are considering switching to 600 milligrams," Sabatine said.
More information
For more on angioplasty, visit the U.S. National Library of Medicine.
Wednesday, March 14, 2007
Women Benefit Less From Clot-Busting Stroke Drug
(HealthDay News) -- Women who suffer strokes are much less likely than men to benefit from treatment with the powerful clot-dissolving drug known as tissue plasminogen activator (tPA), new research suggests.
The biggest such study yet conducted found that while more women survived their stroke after receiving tPA, male patients were more than three times as likely to retain good physical function as measured by a test three months after tPA treatment.
"The most intriguing possibility is that there might be an intrinsic biological difference in the way in which women respond to tPA vs. how men respond to tPA," said Dr. Gary Abrams, an associate professor of neurology at the University of California, San Francisco, and a spokesman for the American Academy of Neurology.
Abrams was not involved in the study, which is published in the March 13 issue of Neurology.
Federal rules mandate that tPA can be used only if treatment starts in the first three hours after a stroke. The drug helps limit brain damage by dissolving clots that block blood flow through arteries.
The trial included almost 1,400 stroke patients, 333 of whom (24 percent) were treated with tPA within three hours.
The study found that 47.5 percent of men getting tPA had good function three months later on a standard measure called the Barthel Index, compared to 30.3 percent of women. On another measure, the Rankin Score, 32.2 percent of men and 23.4 percent of women did well.
"In general, women have worse outcomes than men after a stroke," noted lead researcher Dr. Mitchell S. V. Elkind, an associate professor of neurology at Columbia University, in New York City. "There are potential biological reasons why women may not respond as well as men to tPA. Hormonal factors such as the effects of hormones on blood clots may be the reason."
But Elkind added that, "at this point in time, it is premature to treat women differently [than men] after a stroke. We recommend that women as well as men get to a hospital as quickly as possible and be treated as aggressively, including tPA."
There have been indications that postmenopausal women have higher levels than men of a substance that inhibits tPA activity, Abrams said. "A lot more work would have to be done to prove it, but it is an intriguing thought. But there is conflicting evidence and reasons to believe there are caveats in taking this too far."
The results should also be interpreted cautiously, noted Dr. Edgar J. Kenton III, chair of the American Academy of Neurology's practice committee. "This is the only large trial of the response to tPA in women," he said. "We need more trials proving the point one way or another."
"I don't want this study interpreted to say that women should not get tPA," Kenton stressed. "There are small studies suggesting that with ultra-early treatment -- within one hour -- they do better than men. We need more women in more trials to look at these factors."
Kenton also noted the unusually high percentage of patients in the study who received tPA therapy within the three-hour post-stroke limit recommended by experts.
"Twenty-four percent got tPA within three hours," Kenton noted. "The national average is 5 or 6 percent." The measures used in this trial to get tPA delivered to patients early can and should be applied to everyday practice, he said.
More information
Find out more about tPA at the American Heart Association.
The biggest such study yet conducted found that while more women survived their stroke after receiving tPA, male patients were more than three times as likely to retain good physical function as measured by a test three months after tPA treatment.
"The most intriguing possibility is that there might be an intrinsic biological difference in the way in which women respond to tPA vs. how men respond to tPA," said Dr. Gary Abrams, an associate professor of neurology at the University of California, San Francisco, and a spokesman for the American Academy of Neurology.
Abrams was not involved in the study, which is published in the March 13 issue of Neurology.
Federal rules mandate that tPA can be used only if treatment starts in the first three hours after a stroke. The drug helps limit brain damage by dissolving clots that block blood flow through arteries.
The trial included almost 1,400 stroke patients, 333 of whom (24 percent) were treated with tPA within three hours.
The study found that 47.5 percent of men getting tPA had good function three months later on a standard measure called the Barthel Index, compared to 30.3 percent of women. On another measure, the Rankin Score, 32.2 percent of men and 23.4 percent of women did well.
"In general, women have worse outcomes than men after a stroke," noted lead researcher Dr. Mitchell S. V. Elkind, an associate professor of neurology at Columbia University, in New York City. "There are potential biological reasons why women may not respond as well as men to tPA. Hormonal factors such as the effects of hormones on blood clots may be the reason."
But Elkind added that, "at this point in time, it is premature to treat women differently [than men] after a stroke. We recommend that women as well as men get to a hospital as quickly as possible and be treated as aggressively, including tPA."
There have been indications that postmenopausal women have higher levels than men of a substance that inhibits tPA activity, Abrams said. "A lot more work would have to be done to prove it, but it is an intriguing thought. But there is conflicting evidence and reasons to believe there are caveats in taking this too far."
The results should also be interpreted cautiously, noted Dr. Edgar J. Kenton III, chair of the American Academy of Neurology's practice committee. "This is the only large trial of the response to tPA in women," he said. "We need more trials proving the point one way or another."
"I don't want this study interpreted to say that women should not get tPA," Kenton stressed. "There are small studies suggesting that with ultra-early treatment -- within one hour -- they do better than men. We need more women in more trials to look at these factors."
Kenton also noted the unusually high percentage of patients in the study who received tPA therapy within the three-hour post-stroke limit recommended by experts.
"Twenty-four percent got tPA within three hours," Kenton noted. "The national average is 5 or 6 percent." The measures used in this trial to get tPA delivered to patients early can and should be applied to everyday practice, he said.
More information
Find out more about tPA at the American Heart Association.
Friday, February 02, 2007
The Cardiovascular Cure: How to Strengthen Your Self-Defense Against Heart Attack and Stroke - Book Review
BY JOHN P. COOKE, M.D., PH.D., AND JUDITH ZIMMER; B
ROADWAY BOOKS; $25
SOME MAINSTREAM DOCTORS are bucking the system and suggesting that surgery or drugs may not be the best treatment for stroke, heart disease, and atherosclerosis (hardening of the arteries). One of these doctors, John P. Cooke, M.D., Ph.D., director of the vascular medicine section at Stanford University Medical School in Palo Alto, Calif., has written a book to help us trigger our body's remarkable capacity to heal itself.
Cooke and co-author medical journalist Judith Zimmer explain that a healthy endothelium, the innermost single-cell-thick lining of human blood vessels, releases a substance that packs benefits galore. Called nitric oxide (NO), this substance keeps blood vessels supple, prevents platelets from snagging on vessel walls, hinders the buildup of plaque, and even helps to reduce existing plaque deposits. Cooke says people with heart disease or the risk factors for it have elevated levels of an amino acid that impedes NO production.
To ensure that your endothelium pumps out plenty of NO, Cooke recommends a modified Mediterranean-style diet supplying 1,800 calories a day. The evidence-based diet features whole grains, beans, nuts, legumes, fruits, and vegetables, and emphasizes foods rich in L-arginine, an amino acid used by the endothelium to make NO. His book includes a two-week eating plan with recipes, and detailed information on supplemental nutrients and phytochemicals.
The other component of Cooke's simple plan is aerobic exercise, which increases blood flow through your vessels. Increased blood flow stimulates the production of NO and keeps the endothelium smooth so plaque accumulation is less likely. He advocates at least 30 minutes of aerobic exercise four days a week.
This book manages to be both comprehensive and lively. Cooke presents just the right amount of detail about the scientific underpinnings of his conclusions, which are based on a Nobel-prize-winning theory. He claims you will have vascular improvement in just two weeks--and I believe him.
COPYRIGHT 2002 Weider Publications
COPYRIGHT 2002 Gale Group
ROADWAY BOOKS; $25
SOME MAINSTREAM DOCTORS are bucking the system and suggesting that surgery or drugs may not be the best treatment for stroke, heart disease, and atherosclerosis (hardening of the arteries). One of these doctors, John P. Cooke, M.D., Ph.D., director of the vascular medicine section at Stanford University Medical School in Palo Alto, Calif., has written a book to help us trigger our body's remarkable capacity to heal itself.
Cooke and co-author medical journalist Judith Zimmer explain that a healthy endothelium, the innermost single-cell-thick lining of human blood vessels, releases a substance that packs benefits galore. Called nitric oxide (NO), this substance keeps blood vessels supple, prevents platelets from snagging on vessel walls, hinders the buildup of plaque, and even helps to reduce existing plaque deposits. Cooke says people with heart disease or the risk factors for it have elevated levels of an amino acid that impedes NO production.
To ensure that your endothelium pumps out plenty of NO, Cooke recommends a modified Mediterranean-style diet supplying 1,800 calories a day. The evidence-based diet features whole grains, beans, nuts, legumes, fruits, and vegetables, and emphasizes foods rich in L-arginine, an amino acid used by the endothelium to make NO. His book includes a two-week eating plan with recipes, and detailed information on supplemental nutrients and phytochemicals.
The other component of Cooke's simple plan is aerobic exercise, which increases blood flow through your vessels. Increased blood flow stimulates the production of NO and keeps the endothelium smooth so plaque accumulation is less likely. He advocates at least 30 minutes of aerobic exercise four days a week.
This book manages to be both comprehensive and lively. Cooke presents just the right amount of detail about the scientific underpinnings of his conclusions, which are based on a Nobel-prize-winning theory. He claims you will have vascular improvement in just two weeks--and I believe him.
COPYRIGHT 2002 Weider Publications
COPYRIGHT 2002 Gale Group
The Cardiovascular Cure
The Cardiovascular Cure
Written by John P. Cooke, M.D., Ph.D. and Judith Zimmer
Category: Medical - Diet Therapy
Publisher: BroadwayFormat: Trade Paperback, 336 pagesPub Date: August 2003
Price: $15.95
ISBN: 978-0-7679-0882-5 (0-7679-0882-1)
ABOUT THIS BOOK
The Cardiovascular Cure offers a groundbreaking approach to preventing heart attack and stroke by enhancing your body’s own natural defenses. Dr. John Cooke, head of Stanford Medical School’s vascular unit, has devised a powerful new method for fighting cardiovascular disease without bypass surgery or angioplasty.
Drawing on his own investigations, as well as Nobel Prize-winning research from a team of American scientists, Dr. Cooke provides heart patients with a diet, supplement, and exercise program that will help them feel better in as little as two weeks.
His program also works to prevent heart disease in those at risk.
In 1998, the Nobel Prize in Physiology or Medicine was awarded for the discovery of EDRF (endothelium-derived relaxing factor), a chemical produced in the lining of the blood vessels, which keeps them free of plaque. Dr. Cooke and other investigators have found that specific nutrients can enhance EDRF production and improve blood flow in people with high cholesterol, high blood pressure, diabetes, or other risk factors for heart disease.
This potentially life-saving book shows how anyone can achieve healthier blood vessels (the key to preventing heart disease). A two-week menu plan contains recipes that emphasize EDRF-enhancing foods, and there is detailed information on supplemental nutrients and vitamins that are useful in strengthening the cardiovascular system. Recipes from breakfast (Banana Date-Nut Bread; Blueberry Oat Pancakes; Pineapple Ginger or Tropical Smoothies; Pumpkin Muffins) to dinner (Moroccan Red Snapper; Chicken Wrap with Refried Beans; Soy-Glazed Salmon; Turkey Meatloaf) feature healthy fats found in fish, nuts, and olive oil.
There is also welcome news that red wine and chocolate can be good for you (there are recipes for Double Chocolate Cake and Chocolate Raspberry Surprise). The exercise program consists of the same therapeutic plans Dr. Cooke has prescribed for even his most severely ill patients, many of whom begin to walk and even exercise more vigorously without pain after two weeks. In addition, there are aerobic workouts designed for more active patients.
Dr. Cooke also provides state-of-the-art information (pro and con) on conventional drugs–from aspirin to beta blockers–and medical tests and procedures to further combat cardiovascular disease. With an introduction by Sir John Vane, a Nobel Prize-winning cardiovascular scientist, this book will provide anyone concerned about his or her cardiovascular health with new hope for a pain-free, disease-free life.
From the Hardcover edition.PRAISE“In The Cardiovascular Cure, Dr. Cooke has translated the research of our field into life-saving information that we can all use. If you really care about your cardiovascular health, you must read this book!”--Louis J. Ignarro, Ph.D., 1998 Nobel Laureate in Physiology or Medicine for the discovery of Nitric Oxide“This authoritative book appropriately points out why everyone should worry about the health of their endothelium and, better still, do something to protect it if it shows signs of damage.
Early identification and treatment of reduced nitric oxide release should be the preventive agenda for the new millenium.”--Jay N. Cohn, M.D., Professor of Medicine, University of Minnesota Medical School“This book should be read by all patients with heart disease as well as anyone at increased risk for a heart attack or stroke.
The comprehensive risk reduction program recommended by Dr. Cooke uses the most advanced research to help everyone improve the health of their blood vessels.” --William L. Haskell, Ph.D., Stanford Center for Research in Disease Prevention“The Cardiovascular Cure is a lucidly written description of EDRF and endothelial dysfunction.
Treatment with exercise and a diet rich in arginine, vitamins, and anti-oxidants is important to the many patients prone to develop heart attacks or stroke.”--Dr. Ferid Murad, M.D., Ph.D., Director of the Institute of Molecular Medicine at the University of Texas, 1998 Nobel Laureate in Physiology or Medicine“Helping yourself prevent a heart attack means knowing more than your ‘cholesterol count.’
In this clearly written book, Dr. Cooke introduces you to the important role played by the endothelium (the lining of your blood vessels) in this process, and what you can do to keep this vital organ as healthy as possible.”--Gerald Reaven, Professor of Medicine, Stanford University School of MedicineFrom the Hardcover edition.
ABOUT THIS AUTHORJOHN P. COOKE, M.D., Ph.D., is Associate Professor of Medicine and Director of the Section of Vascular Medicine at Stanford University’s Medical School. He trained at the Mayo Clinic, earning a Ph.D. in physiology there, and he was on the faculty of Harvard Medical School before he was recruited to Stanford to spearhead the program in Vascular Biology and Medicine.
He is a sought-after consultant and has served on numerous national and international committees dealing with cardiovascular diseases, including those of the American Heart Association and the National Heart, Lung and Blood Institute. JUDITH ZIMMER has been a medical journalist for more than fifteen years.
She has contributed to such publications as the New York Times, and Self and Fitness magazines, and she currently writes for academic medical centers in New York City.
From the Hardcover edition.
{kind=link}
Written by John P. Cooke, M.D., Ph.D. and Judith Zimmer
Category: Medical - Diet Therapy
Publisher: BroadwayFormat: Trade Paperback, 336 pagesPub Date: August 2003
Price: $15.95
ISBN: 978-0-7679-0882-5 (0-7679-0882-1)
ABOUT THIS BOOK
The Cardiovascular Cure offers a groundbreaking approach to preventing heart attack and stroke by enhancing your body’s own natural defenses. Dr. John Cooke, head of Stanford Medical School’s vascular unit, has devised a powerful new method for fighting cardiovascular disease without bypass surgery or angioplasty.
Drawing on his own investigations, as well as Nobel Prize-winning research from a team of American scientists, Dr. Cooke provides heart patients with a diet, supplement, and exercise program that will help them feel better in as little as two weeks.
His program also works to prevent heart disease in those at risk.
In 1998, the Nobel Prize in Physiology or Medicine was awarded for the discovery of EDRF (endothelium-derived relaxing factor), a chemical produced in the lining of the blood vessels, which keeps them free of plaque. Dr. Cooke and other investigators have found that specific nutrients can enhance EDRF production and improve blood flow in people with high cholesterol, high blood pressure, diabetes, or other risk factors for heart disease.
This potentially life-saving book shows how anyone can achieve healthier blood vessels (the key to preventing heart disease). A two-week menu plan contains recipes that emphasize EDRF-enhancing foods, and there is detailed information on supplemental nutrients and vitamins that are useful in strengthening the cardiovascular system. Recipes from breakfast (Banana Date-Nut Bread; Blueberry Oat Pancakes; Pineapple Ginger or Tropical Smoothies; Pumpkin Muffins) to dinner (Moroccan Red Snapper; Chicken Wrap with Refried Beans; Soy-Glazed Salmon; Turkey Meatloaf) feature healthy fats found in fish, nuts, and olive oil.
There is also welcome news that red wine and chocolate can be good for you (there are recipes for Double Chocolate Cake and Chocolate Raspberry Surprise). The exercise program consists of the same therapeutic plans Dr. Cooke has prescribed for even his most severely ill patients, many of whom begin to walk and even exercise more vigorously without pain after two weeks. In addition, there are aerobic workouts designed for more active patients.
Dr. Cooke also provides state-of-the-art information (pro and con) on conventional drugs–from aspirin to beta blockers–and medical tests and procedures to further combat cardiovascular disease. With an introduction by Sir John Vane, a Nobel Prize-winning cardiovascular scientist, this book will provide anyone concerned about his or her cardiovascular health with new hope for a pain-free, disease-free life.
From the Hardcover edition.PRAISE“In The Cardiovascular Cure, Dr. Cooke has translated the research of our field into life-saving information that we can all use. If you really care about your cardiovascular health, you must read this book!”--Louis J. Ignarro, Ph.D., 1998 Nobel Laureate in Physiology or Medicine for the discovery of Nitric Oxide“This authoritative book appropriately points out why everyone should worry about the health of their endothelium and, better still, do something to protect it if it shows signs of damage.
Early identification and treatment of reduced nitric oxide release should be the preventive agenda for the new millenium.”--Jay N. Cohn, M.D., Professor of Medicine, University of Minnesota Medical School“This book should be read by all patients with heart disease as well as anyone at increased risk for a heart attack or stroke.
The comprehensive risk reduction program recommended by Dr. Cooke uses the most advanced research to help everyone improve the health of their blood vessels.” --William L. Haskell, Ph.D., Stanford Center for Research in Disease Prevention“The Cardiovascular Cure is a lucidly written description of EDRF and endothelial dysfunction.
Treatment with exercise and a diet rich in arginine, vitamins, and anti-oxidants is important to the many patients prone to develop heart attacks or stroke.”--Dr. Ferid Murad, M.D., Ph.D., Director of the Institute of Molecular Medicine at the University of Texas, 1998 Nobel Laureate in Physiology or Medicine“Helping yourself prevent a heart attack means knowing more than your ‘cholesterol count.’
In this clearly written book, Dr. Cooke introduces you to the important role played by the endothelium (the lining of your blood vessels) in this process, and what you can do to keep this vital organ as healthy as possible.”--Gerald Reaven, Professor of Medicine, Stanford University School of MedicineFrom the Hardcover edition.
ABOUT THIS AUTHORJOHN P. COOKE, M.D., Ph.D., is Associate Professor of Medicine and Director of the Section of Vascular Medicine at Stanford University’s Medical School. He trained at the Mayo Clinic, earning a Ph.D. in physiology there, and he was on the faculty of Harvard Medical School before he was recruited to Stanford to spearhead the program in Vascular Biology and Medicine.
He is a sought-after consultant and has served on numerous national and international committees dealing with cardiovascular diseases, including those of the American Heart Association and the National Heart, Lung and Blood Institute. JUDITH ZIMMER has been a medical journalist for more than fifteen years.
She has contributed to such publications as the New York Times, and Self and Fitness magazines, and she currently writes for academic medical centers in New York City.
From the Hardcover edition.
Monday, January 29, 2007
Calculator Helps Users Gauge Heart Attack Risk
 (HealthDay News) -- A new online heart disease risk calculator that can help you understand and gauge your heart attack risk is available from the Mayo Clinic.
(HealthDay News) -- A new online heart disease risk calculator that can help you understand and gauge your heart attack risk is available from the Mayo Clinic.The risk calculator on MayoClinic.com asks several questions about your lifestyle and health and then determines your 10-year risk of a heart attack. The risk score is based on a number of factors, such as age, gender, tobacco use, cholesterol levels, and blood pressure.
You can find the risk calculator by heading to MayoClinic.com and looking under "Heart Disease Risk Factors," in the Web site's Heart Disease Center.
About one in 10 people with a risk level of 12 percent will have a heart attack or die of heart disease within the next 10 years, experts say.
Here are five heart disease prevention tips:
- Don't smoke or use tobacco products.
- Get exercise. Regular, moderately vigorous physical activity can reduce the risk of fatal heart disease by 25 percent. Combining physical activity with other positive lifestyle habits, such as maintaining a health weight, can provide even more heart health benefits.
- Eat a heart-healthy diet that includes plenty of fruits, vegetables, whole grains, and low-fat dairy products. Legumes, low-fat sources of protein and certain types of fish may also help reduce heart disease risk.
- Limit intake of saturated fats and trans fat.
- Watch your weight.
- Excess pounds can lead to conditions -- high blood pressure, high cholesterol and diabetes -- that increase the risk of heart disease.
- Get regular blood pressure and cholesterol screenings.
- High blood pressure and high cholesterol can damage your cardiovascular system, including your heart.
More information
There's more on reducing heart disease risk factors at the American Heart Association.
Thursday, December 07, 2006
FDA Panel to Weigh Value of Drug-Coated Stents
(HealthDay News) -- When a U.S. Food and Drug Administration advisory committee begins a two-day session Thursday to examine the safety of drug-coated stents, thousands of cardiologists and millions of patients will be paying close attention.
Coated stents have dominated cardiovascular surgery since their introduction several years ago. Some 2 million to 3 million people in the United States now carry one of these devices in an artery, according to the latest FDA estimates, with implantations topping 900,000 per year.
But a number of studies have now suggested that these coated stents, which can cost thousands of dollars each, have long-term dangers -- most specifically, the risk of thrombotic artery blockages that can cause heart attacks. So, cardiologists are trying to assess the risk vs. benefit equation for coated stents.
That means that this week's meeting "will be a very closely watched panel," said Dr. Deepak Bhatt, an interventional cardiologist at the Cleveland Clinic. "Cardiologists are looking for guidance and will be very receptive to whatever comes out of that meeting."
But the controversy is already affecting medical practice, Bhatt said. His team published a study that found a slight increase in thrombotic events -- about 0.5 percent -- in patients getting coated rather than bare-metal stents.
So, Bhatt has cut back on his use of coated stents, "probably from 90 percent to 80 percent of my patients." And, he said, other cardiologists are being "a little more cautious about the implants or are extending the duration of anti-clotting medications."
Anti-clotting medications such as Plavix (clopidogrel) and aspirin are important because doctors often prescribe them after stent implantation. And research published earlier this week linked the increased risk of thrombosis to discontinuation of one such drug, Plavix.
"This raises the question of whether these drug-eluting stents should be anticoagulated for a long period of time," noted Dr. John Kao, assistant professor of medicine at the University of Illinois at Chicago. "What that time period is, is at this moment unclear."
The American Heart Association released a cautious statement saying that "there is conflicting data regarding the magnitude and significance" of the increased risk of late thrombosis in patients getting coated stents.
What is clear is that "it is very important that patients do not discontinue their anti-platelet therapy within a year after stenting without consulting their treating cardiologist," the heart association statement said. The risk of discontinuing Plavix therapy is less clear, it said.
"Additional studies probably will be required to define the risk of late blood clots in patients with drug-eluting stents and the appropriate therapy to prevent them," the association statement said.
There are other angles to the drug-coated stent issue. Stenting and its follow-up treatment is now a very big business. Two brands of drug-coated stents are sold in the United States -- one, brand-named Taxus, is marketed by Boston Scientific Corp., while another, Cypher, is made by Cordis Corp., a subsidiary of Johnson & Johnson. And a number of physicians invited to participate in the FDA advisory committee have ties to one or another of these companies.
For example, one panel member is Dr. Robert A. Harrington, who heads a research unit at Duke University that gets funding from Boston Scientific and Johnson & Johnson.
In all, six of the experts summoned by the FDA have such ties to heart device manufacturers.
However, Dr. Daniel Schultz, director of the FDA's Center for Devices and Radiological Health, defended the composition of the group during a news conference Tuesday.
"Whether or not waivers were granted or not granted, it was important that we had a panel of individuals who were able to give us objective, non-biased information," Schultz said. "Looking at the entire panel, if you look at that objectively, you will see that we have done a pretty good job of achieving that goal."
Another issue: the cost to patients of Plavix, which can total $120 or more a month. Current guidelines recommend that Plavix be taken (along with aspirin) for three months if a Boston Scientific coated stent is implanted and for six months with a Cordis stent. Because the drug can be so expensive, Kao said he sometimes makes his decisions on implanting a bare-metal or coated stent on the basis of a patient's income.
"When I evaluate someone who needs intervention who is on a fixed income and cannot afford to take Plavix for six to 12 months, I put in a bare-metal stent," Kao said.
For patients who can afford the drug, "my recommendation now is to take it for one year, indefinitely if they can afford it," he said.
But there are medical considerations in prescribing Plavix, Bhatt said. The medication can cause dangerous bleeding, he said, so he evaluates patients for bleeding risk before prescribing the drug.
Cardiologists in Europe now are "a little more cautious about extending the duration of anti-clotting medications," and the same is becoming true in the United States, Bhatt said.
The issue of possible clots is not the only consideration when weighing the need for drug-coated stents, said Dr. Joseph B. Muhlestein, a professor of medicine at the University of Utah. His group has followed patients receiving stents very carefully and has found "something we don't understand," he said.
As expected, the drug-coated stents did reduce the incidence of artery closure at the site where they were implanted, Muhlestein said. But the incidence of artery problems at other sites occurred "significantly more often than when we used bare-metal stents," he said. So, the overall incidence of artery problems ended up being the same, regardless of stent type, Muhlestein said.
It is possible that the problem occurred because coated stents were used on more high-risk patients, he said. But it's also possible that the coated stents interfered with the endothelium, the delicate tissue that lines the arteries -- something also reported in a Dutch study.
These doubts about the value of coated stents have caused Muhlestein to cut back on their use. "We used to use them in 90 percent of cases," he said. "Now, it's about 40 percent."
What does all of this mean for someone facing a stent implant? "At this point, in the absence of more information, the kind of stent should be the subject of discussion between patients and cardiologists," advised Dr. David F. Kong, an assistant professor of medicine at Duke University.
More information
To learn more on stents, head to the American Heart Association.
Coated stents have dominated cardiovascular surgery since their introduction several years ago. Some 2 million to 3 million people in the United States now carry one of these devices in an artery, according to the latest FDA estimates, with implantations topping 900,000 per year.
But a number of studies have now suggested that these coated stents, which can cost thousands of dollars each, have long-term dangers -- most specifically, the risk of thrombotic artery blockages that can cause heart attacks. So, cardiologists are trying to assess the risk vs. benefit equation for coated stents.
That means that this week's meeting "will be a very closely watched panel," said Dr. Deepak Bhatt, an interventional cardiologist at the Cleveland Clinic. "Cardiologists are looking for guidance and will be very receptive to whatever comes out of that meeting."
But the controversy is already affecting medical practice, Bhatt said. His team published a study that found a slight increase in thrombotic events -- about 0.5 percent -- in patients getting coated rather than bare-metal stents.
So, Bhatt has cut back on his use of coated stents, "probably from 90 percent to 80 percent of my patients." And, he said, other cardiologists are being "a little more cautious about the implants or are extending the duration of anti-clotting medications."
Anti-clotting medications such as Plavix (clopidogrel) and aspirin are important because doctors often prescribe them after stent implantation. And research published earlier this week linked the increased risk of thrombosis to discontinuation of one such drug, Plavix.
"This raises the question of whether these drug-eluting stents should be anticoagulated for a long period of time," noted Dr. John Kao, assistant professor of medicine at the University of Illinois at Chicago. "What that time period is, is at this moment unclear."
The American Heart Association released a cautious statement saying that "there is conflicting data regarding the magnitude and significance" of the increased risk of late thrombosis in patients getting coated stents.
What is clear is that "it is very important that patients do not discontinue their anti-platelet therapy within a year after stenting without consulting their treating cardiologist," the heart association statement said. The risk of discontinuing Plavix therapy is less clear, it said.
"Additional studies probably will be required to define the risk of late blood clots in patients with drug-eluting stents and the appropriate therapy to prevent them," the association statement said.
There are other angles to the drug-coated stent issue. Stenting and its follow-up treatment is now a very big business. Two brands of drug-coated stents are sold in the United States -- one, brand-named Taxus, is marketed by Boston Scientific Corp., while another, Cypher, is made by Cordis Corp., a subsidiary of Johnson & Johnson. And a number of physicians invited to participate in the FDA advisory committee have ties to one or another of these companies.
For example, one panel member is Dr. Robert A. Harrington, who heads a research unit at Duke University that gets funding from Boston Scientific and Johnson & Johnson.
In all, six of the experts summoned by the FDA have such ties to heart device manufacturers.
However, Dr. Daniel Schultz, director of the FDA's Center for Devices and Radiological Health, defended the composition of the group during a news conference Tuesday.
"Whether or not waivers were granted or not granted, it was important that we had a panel of individuals who were able to give us objective, non-biased information," Schultz said. "Looking at the entire panel, if you look at that objectively, you will see that we have done a pretty good job of achieving that goal."
Another issue: the cost to patients of Plavix, which can total $120 or more a month. Current guidelines recommend that Plavix be taken (along with aspirin) for three months if a Boston Scientific coated stent is implanted and for six months with a Cordis stent. Because the drug can be so expensive, Kao said he sometimes makes his decisions on implanting a bare-metal or coated stent on the basis of a patient's income.
"When I evaluate someone who needs intervention who is on a fixed income and cannot afford to take Plavix for six to 12 months, I put in a bare-metal stent," Kao said.
For patients who can afford the drug, "my recommendation now is to take it for one year, indefinitely if they can afford it," he said.
But there are medical considerations in prescribing Plavix, Bhatt said. The medication can cause dangerous bleeding, he said, so he evaluates patients for bleeding risk before prescribing the drug.
Cardiologists in Europe now are "a little more cautious about extending the duration of anti-clotting medications," and the same is becoming true in the United States, Bhatt said.
The issue of possible clots is not the only consideration when weighing the need for drug-coated stents, said Dr. Joseph B. Muhlestein, a professor of medicine at the University of Utah. His group has followed patients receiving stents very carefully and has found "something we don't understand," he said.
As expected, the drug-coated stents did reduce the incidence of artery closure at the site where they were implanted, Muhlestein said. But the incidence of artery problems at other sites occurred "significantly more often than when we used bare-metal stents," he said. So, the overall incidence of artery problems ended up being the same, regardless of stent type, Muhlestein said.
It is possible that the problem occurred because coated stents were used on more high-risk patients, he said. But it's also possible that the coated stents interfered with the endothelium, the delicate tissue that lines the arteries -- something also reported in a Dutch study.
These doubts about the value of coated stents have caused Muhlestein to cut back on their use. "We used to use them in 90 percent of cases," he said. "Now, it's about 40 percent."
What does all of this mean for someone facing a stent implant? "At this point, in the absence of more information, the kind of stent should be the subject of discussion between patients and cardiologists," advised Dr. David F. Kong, an assistant professor of medicine at Duke University.
More information
To learn more on stents, head to the American Heart Association.
Thursday, November 16, 2006
VasuFlex is a proprietary formula based on this exciting research.
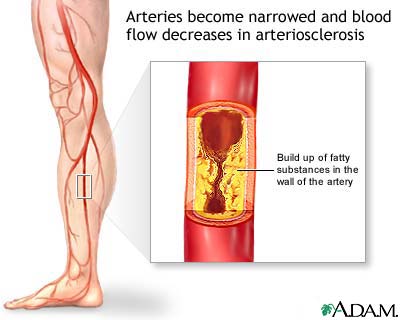 According to Nobel Laureate, Dr. Ignarro, this balanced combination of amino acids can increase the body's ability to prevent and even reverse cardiovascular disease.
According to Nobel Laureate, Dr. Ignarro, this balanced combination of amino acids can increase the body's ability to prevent and even reverse cardiovascular disease.The extraordinary research of three American Doctors indicates that a power packed combination of nutritional supplements can work to improve the function of the inner lining of the blood vessels and aid in boosting the production of nitric oxide (NO), the agent in your body that widens blood vessels and increases blood flow.
New Spirit Naturals' proprietary formula includes important supportive nutrients that further enhance the synthesis and/or prevent the breakdown of nitric oxide.
New Spirit Naturals is a brand you can trust for quality.
As we age, our risk increases
 With aging, arteries lose elasticity, often triggering elevated blood pressure.
With aging, arteries lose elasticity, often triggering elevated blood pressure.Dietary abuses and a sedentary lifestyle further impact the health of our vascular system.
Recent Nobel Prize Winning Research is literally changing the landscape of cardiovascular health and reminding us of the power of the body to heal itself if provided the right nutrients.
Subscribe to:
Posts (Atom)
Dr. Group's Secret to Health Kit$39.94  Dr. Group's Secret to Health Kit offers simple at-home solutions for cleansing internally and externally thereby reducing toxins, restoring the body's natural healing process, and helping you achieve true health and happiness. |